
Can it be harmful to view your MRI report? Clearly the answer is yes. Maybe not for all of you… but certainly for a good number of you. I have seen many people significantly curtail their activities because of something they saw on an MRI report. The MRI report might have been discussing a normal “age-appropriate” finding, but you can’t get past the fact that something was listed as being “torn.” What’s the downstream cost of a self-imposed limited quality of life — the loss of something you enjoyed doing— and an associated decrease in your physical fitness?
“You cannot unsee your MRI report.”
Robert was a pleasant and very active 52-year-old. He coached soccer, and he was an accomplished trail runner. That’s how we met. He was super fast, and that helped me. He loved climbing hills as much as I did. These weekend runs together helped both of us more than we would ever know. I might be very winded while ascending a steep hill that didn’t appear to bother him. But I wasn’t going to stop :-).
Almost no one over 40 will have a “normal” MRI report of the shoulder, knee, spine, or hip. Many of the changes seen on an MRI are considered to be “age-appropriate” changes to some of the structures in these joints. Most of those changes can be ignored and will not impact on your activities.
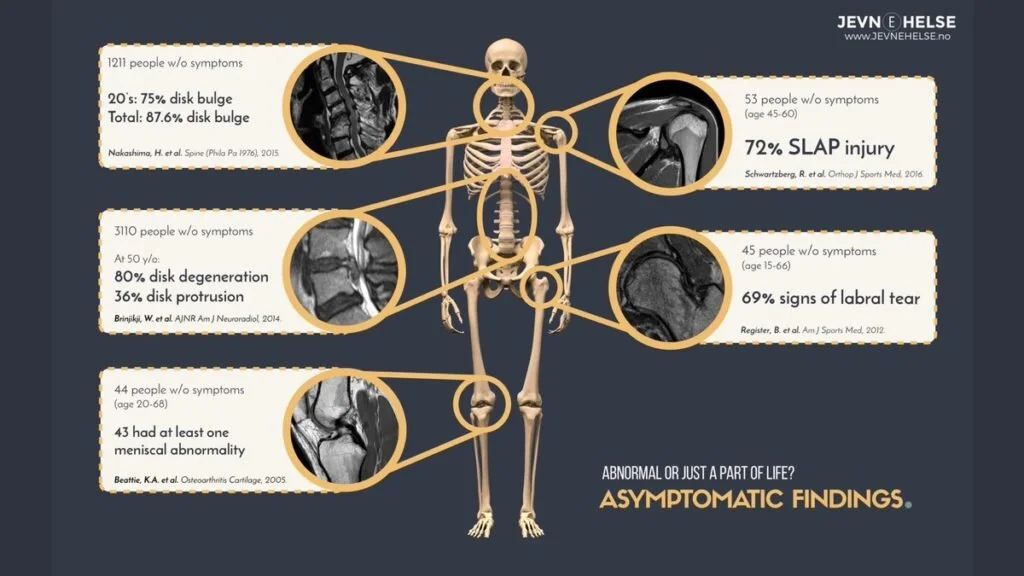
This graphic shows the MRI findings of active people without joint pain.
87% of people without back pain have disc bulges
72% had a labral tear (SLAP tear) in their shoulder
Nearly 50% had knee meniscus findings.
69% had a labral tear in their hip.
Imagine this scenario. Your shoulder has a labral tear in it. You just don’t know it. Upwards of 70% of adults will have a labral tear on their MRI—even if they have NO PAIN. So, you have a labral tear… you’re playing tennis, you’re active with your children and you workout in the gym regularly. Two years later you wake up with an ache in the shoulder. You have an MRI, and they find that labral tear. Is that tear, which has been there for years, or decades, a cause of your pain? Probably not. But your mind will assume that it is. Will that affect your decision making about going to the gym? Playing tennis? It might.
We discussed MRI findings in normal shoulders in this post.
Middle-aged patients with shoulder pain presumed to be due to a small rotator cuff tear have been studied. It turns out, if you MRI their other shoulder, which is not painful, we will often find the same size tear! Why are we saying that one tear hurts, but one tear doesn’t? Again, is the tear the cause of pain? We do not know. Bear with me…
Sometimes an MRI can complicate decision making more than it helps.

Robert’s shoulder had been bothering him for a week or so. We had discussed it during one of our runs. Given his lack of injury, I suggested waiting it out for a while. But like many of us, he didn’t think that pain was normal at our age. Even though his pain was “mild” and didn’t affect his activities, or affect his sleep, the thought that something might be wrong bothered him. “Pain can’t be normal… can it”?
We are an over-diagnosed society: Too many MRIs are performed each year.
Millions of MRI scans are performed in the US each year. The cost is astronomical. And as we will explore, that cost involves more than actual dollars spent. We are spending upwards of $25,000 a year for a family insurance policy. If you do not think that the current over-imaging environment is contributing to that, you would be wrong.
How many of you insisted on an MRI, and by the time you went to review the results with your doctor, the pain was starting to improve already? Despite feeling better, you cannot unsee your MRI results.
Many physicians will likely find it easier to MRI a joint that hurts, rather than take the time to explain why it isn’t necessary. Time is money. Healthcare is a business. Another issue, physicians are rated by their employers by their patient satisfaction scores. Saying no to a patient who adamantly insists on an MRI might negatively affect that score.
Robert decided to see his primary care doctor about his shoulder. While at his primary care doctor’s office, he insisted on having an MRI. That was a fact he boasted about when he called me later that night. Tough guys don’t always finish first.
Robert’s MRI showed a tiny rotator cuff tear and some inflammation. This is often what a shoulder MRI of an active 50 something shows. Robert picked up his MRI report before his doctor had a chance to call him. He went straight to Google and read all that he could about rotator cuff tears.
Robert lacked the knowledge necessary to put the results into perspective. Context matters.
Was the tear acute?
Was it chronic?
Was the cuff tissue thin?
Did he have a cable dominant cuff pattern?
Was there tendinosis?
Any associated muscle atrophy?
Any tendon retraction?
These are issues that shoulder surgeons think about when we view the MRI images. Not all radiologists know this… so it might not be addressed in your MRI report.
Robert’s doctor called him the next day. His doctor wasn’t sure about how to handle this finding on his shoulder MRI, so he referred Robert to a specialist.
The following Saturday, Robert and I were supposed to run together. He didn’t want to go. He didn’t have a game to coach. His legs felt great. He was afraid of hurting his shoulder more. That might seem to be intuitive. I tried to convince him to run, but I wasn’t his doctor, so I ran alone that fine day.
Robert saw a local Orthopedic Surgeon. Without even examining him, Robert was told he needed surgery. Yes, some docs might treat an MRI report finding. How was my friend to know that these tears usually don’t require surgery? That’s what his doctor was supposed to tell him. But we are experiencing a high-tech low-touch evolution in health care. The art of the physical exam is being lost. The art of listening to people and educating them about their choices based on everything they shared with us and their imaging findings is at risk of being lost too.
Healthcare is an RVU/productivity driven world. It is a fee for service world. The more services, the higher the fees. It pays to keep that in mind when you are told that you need to have something done.
Robert had his surgery. It didn’t go well. His pain persisted, and he also developed a frozen shoulder. After six months of stretching exercises, and costly physical therapy, his range of motion returned to normal, but he still had pain. Now he wasn’t sleeping well. He hadn’t been running in 8 months, he gained 25 pounds, and he wasn’t the same guy I knew a year ago.
Robert’s pain eventually subsided, but the damage was done. Is this an extreme case? Perhaps. Is this a rare problem? No.
YOU CANT UNSEE YOUR MRI REPORT
Insisting on an MRI of a joint that just started bothering you isn’t always the right answer. We often know which shoulder or knee requires an MRI. Many of the findings that show up on our imaging studies are “normal” for our age. You often do not need to curtail your activities at all. Quite often, the pain will subside if you wait long enough. Our wonderful physical therapy colleagues are very successful at crafting a rehabilitation program to assist you in feeling better.
An MRI is necessary if it might affect our treatment plan. Otherwise, there is no rush to crawl inside a magnet. Trust that your doctor often knows what findings to look for on your examination to determine if an MRI is necessary. Even if those findings aren’t present, we will order an MRI if your pain doesn’t improve with time, medications, and physical therapy. Walking into an office and demanding an MRI might start you down a path that you do not want to go down.
Disclaimer: this information is for your education and should not be considered medical advice regarding diagnosis or treatment recommendations. Some links on this page may be affiliate links. Read the full disclaimer.