




Golf is now as bad for participants as a CONTACT sport say experts probing an epidemic of bad backs among professionals
Focus on strength over style making spinal injuries common among golf players
More than a third of weekend enthusiasts suffering along with half professionals
Tiger Woods, Phil Mickelson, Justin Rose and Rory McIlroy among those suffered
Modern golf has triggered an epidemic of back pain among players, according to new research.
A focus on strength over style is making spinal injuries common among both amateurs and professionals.
More than half of those who golf for a living suffer from back injuries, with a third of weekend enthusiasts falling victim to similar conditions.
Global superstars Tiger Woods, Phil Mickelson, Justin Rose and Rory McIlroy are among those whose careers have been blighted by the issue.
The sport is extremely exerting and even endangering to public health, scientists say.
A focus on strength over style is making spinal injuries common among both amateurs and professionals (Pictured, Rory McIlroy)

Rory MCIlroy
Dr Corey Walker, of Barrow Neurological Institute in Phoenix, Arizona, said: 'Among professional and amateur golfers, back disorders remain the most common injury, comprising 55 per cent and 35 per cent of injuries in these groups, respectively.'
Household names like McIlroy and Britain's world number one Rose now experience spinal problems at far younger ages than the general population.
Dr Walker compared the swing of today's professionals - such as Woods - with those of past legends like Jack Nicklaus and Ben Hogan.
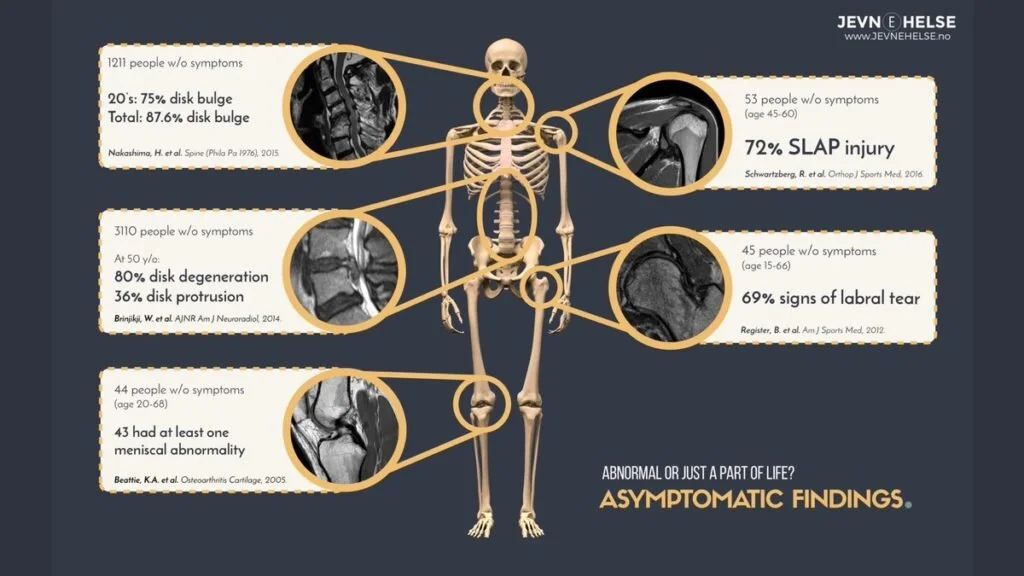
A golf swing causes the spine to rotate at a tilt repeatedly which then stresses the backbone.
This repeated stress has now led to a condition dubbed 'repetitive traumatic discopathy' or RTD.
This is further stressed when players participate in intensive strength-training sessions.
During the down swing, greater force is directed toward the spinal disc and joints which makes them crooked.
A previous study of Japanese professional golfers demonstrated this for the first time on X-Ray images.
Dr Walker said: 'We too have seen this within our practice among elite golfers seeking consultation for back pain.'
With more than 300 swings a day the golfer experiences minor traumatic injuries to the spinal discs. Over time this can result in RTD.

Tiger Woods
4 back surgeries
More than half of those who golf for a living suffer from back pain, with a third of weekend enthusiasts falling victim to similar conditions (Pictured, Tiger Woods)
Dr Walker believes biomechanics and extra gym sessions explain the growing number of injuries - especially among younger players.
The findings, published in the Journal of Neurosurgery: Spine, could now lead to better treatments.
Dr Walker said: 'While seemingly innocuous at first glance, the forces necessary to generate swing speeds that allow golfers to hit the ball at their current distances are significant and place extraordinary loading and torsional stress on the spine.'
Some estimates indicate professionals experience about 7,500 Newtons of compressive force during the downswing - eight times the average human body weight.
Dr Walker said: 'The long-term effects are not trivial - particularly for a sport that allows for decades of participation.
'As technology has propelled driving distances forward, so too has the focus on creating swing paths that produce the most power.
'To achieve the acceleration required for club head speeds greater than 100 mph in one-fifth of a second, a slow deliberate backswing is followed by an explosive rotational downswing.
'By rotating their hips, shoulders, and hands backward, players generate wound-up, spring-like potential energy that is then released in a concentric movement as the club comes back down.
'During this phase, the hips slide forward - hence the phrase 'leading with the hips' - and both hips and shoulders twist toward the target to pull the club into the follow-through.'
The intervertebral discs act as 'cushions' between the spinal bones.
Discopathy causes them to lose flexibility, elasticity and shock-absorbing characteristics.
The outer fibres that surround the disc become brittle and are more easily torn. At the same time the gel at the centre of the disc dries out and shrinks.

Justin Rose
Global superstars Tiger Woods, Phil Mickelson, Justin Rose (pictured) and Rory McIlroy are among those whose careers have been blighted by the issue
The biggest hitters could be most at risk. McIlroy once hit the ball a whopping 436 yards off the tee at the Scottish Open - twice that of an average club hacker.
But to illustrate how injury can occur the researchers chronicled Woods' years of debilitating spine pain.
He holds the record for a drive on the US PGA tour - blasting the ball 498-yards on the 18th at Kapalua, Hawaii, during the 2002 Tournament of Champions.
Dr Walker said: 'We believe Tiger Woods' experience with spinal disease highlights a real and under-recognised issue amongst modern era golfers.'
Last year, the 43 year-old returned to the game after three operations on his incapacitating back that began in 2014 - claiming to be finally pain free and a 'walking miracle.'
Dr Walker said: 'His victory at the Tour Championship may be considered one of the greatest comebacks in all of sports history.'
In the US alone nearly 32 million people play golf - one-in-ten of the population.
In the UK about 1.5 million adults play at least once a week - almost twice the participation rate of tennis.
Dr Walker said: 'As spine surgeons, we appreciate golf's impact on spinal health.
'RTD results from years of degenerative 'hits' or strains on the spine resulting in early onset breakdown, instability and pain.
'We hope medical practitioners - and surgeons in particular - will be able to diagnose and treat golfers with RTD in a specialized fashion going forward.'